

Medically reviewed by Mr Amer Raza MBBS MRCOG, GMC 5205372 | Last reviewed: 8 June 2026
Key Facts: Heavy periods affect around one in three women and are defined as losing more than 80ml of blood per cycle or bleeding lasting longer than seven days. Common causes include fibroids, adenomyosis and hormonal imbalance. Effective treatment is available, and no GP referral is needed for a private assessment.
Heavy menstrual bleeding can disrupt work, sleep, social life and emotional wellbeing. Whether you are experiencing occasional heavy cycles or a clear change in your normal pattern, understanding the underlying cause is the first step towards effective treatment.
At Ovara Health in Chelsea, Mr Amer Raza offers specialist gynaecology assessment for women with heavy periods. Appointments are available without a GP referral, with prompt access to investigation and a personalised treatment plan.
What causes heavy periods?
Heavy menstrual bleeding rarely occurs without an underlying reason. Identifying the cause guides the most appropriate treatment and avoids unnecessary delays in management.
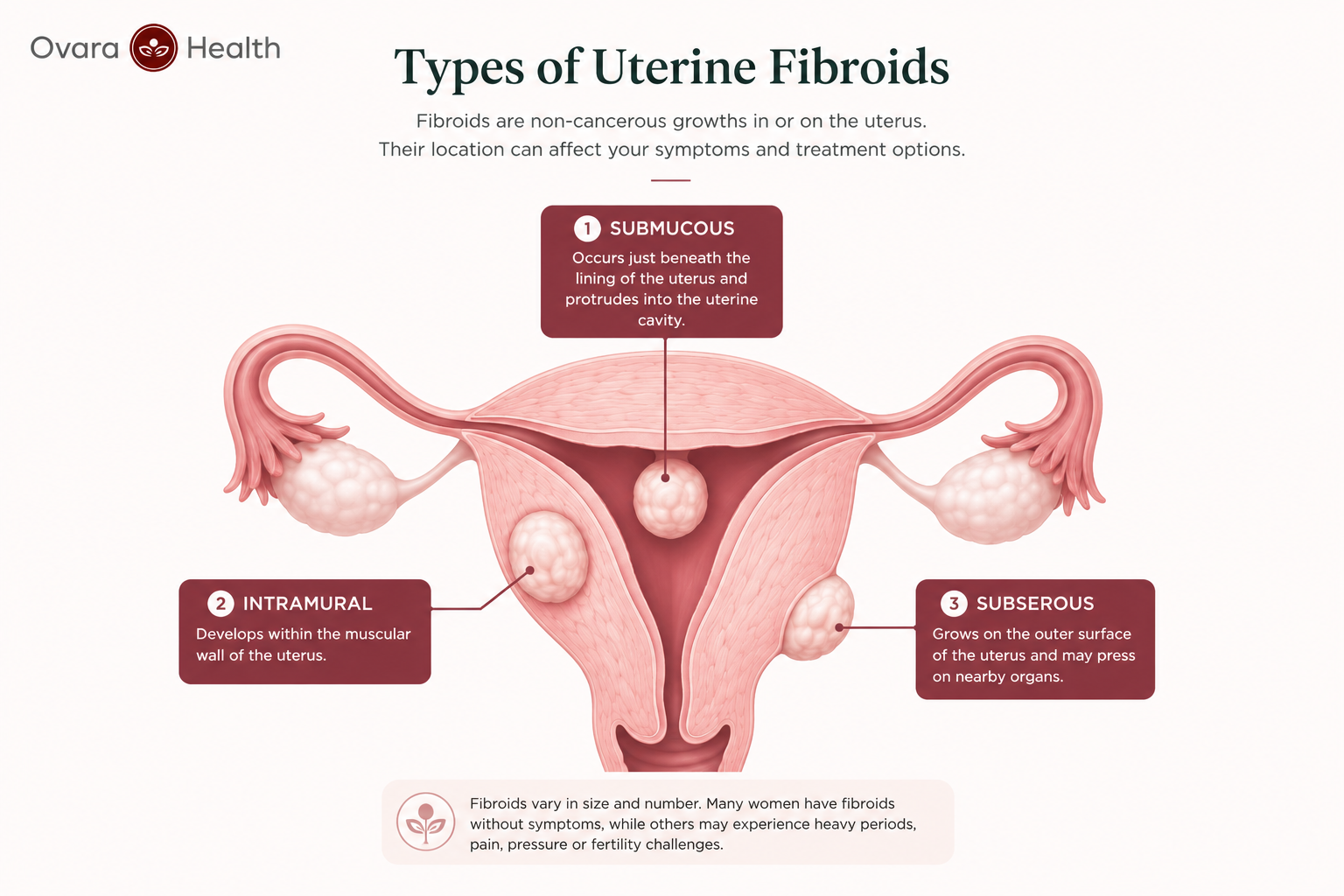
Uterine fibroids
Fibroids are the most common structural cause of heavy periods. These non-cancerous growths within or around the uterine wall can significantly increase menstrual blood loss and prolong bleeding. Submucous fibroids, which grow into the uterine cavity, are particularly associated with heavy and irregular cycles.
Hormonal imbalance
An imbalance between oestrogen and progesterone can cause the uterine lining to thicken more than usual, leading to heavier bleeding when it sheds. This is especially common during perimenopause and in conditions such as polycystic ovary syndrome (PCOS).
Adenomyosis
Adenomyosis occurs when the tissue that normally lines the uterus grows into the muscular wall of the womb. It causes the uterus to enlarge and typically results in heavy, painful and prolonged periods. It is frequently underdiagnosed and can significantly impact quality of life.
Endometrial polyps
Polyps are small benign growths on the lining of the uterus. Although usually non-cancerous, they can cause heavy and irregular bleeding. They are typically identified on ultrasound or during hysteroscopy.
Thyroid disorders
An underactive thyroid (hypothyroidism) affects menstrual cycle regularity and flow. Women with undiagnosed or poorly controlled hypothyroidism often experience heavier, more frequent periods alongside fatigue, weight gain and feeling cold.
Other causes
Bleeding disorders such as von Willebrand disease, certain medications including anticoagulants, and in rare cases endometrial changes may also contribute to heavy menstrual bleeding. A thorough assessment helps identify or exclude these less common causes.
Heavy periods for 2 weeks — when should you be concerned?
Menstrual bleeding that lasts longer than seven days, or that continues well beyond your normal cycle, warrants medical assessment. Two weeks of continuous bleeding should not be dismissed as simply a bad month.
What counts as a heavy period?
Medically, heavy menstrual bleeding is defined as blood loss of more than 80ml per cycle or bleeding lasting longer than seven days. Useful practical markers include needing to change a pad or tampon every one to two hours, passing clots larger than a 50p coin or bleeding that soaks through clothing or bedding.
The impact of prolonged heavy bleeding
Extended heavy bleeding depletes iron stores and can lead to iron deficiency anaemia, causing fatigue, breathlessness, dizziness and difficulty concentrating. Many women live with anaemia for months without realising it. If you feel persistently tired alongside heavy bleeding, blood tests to check your iron levels are an important part of assessment.
When to seek assessment
Seek a specialist review if your periods last longer than seven days, if bleeding is heavy enough to disrupt daily activity or if your cycle has recently changed without an obvious explanation. Any bleeding between periods, after sex or — for women over 45 — a new pattern of heavy bleeding should also be assessed without delay.
Concerned about heavy periods? You do not need a GP referral to be seen at Ovara Health. Call us on 0207 751 4488 or book online for a prompt private gynaecology assessment in Chelsea.
What should I do with heavy periods?
If heavy periods are affecting your quality of life, taking action early leads to better outcomes. There are practical steps you can take while awaiting assessment, and clear signs that indicate when professional evaluation is needed.
Keep a symptom diary
Recording your cycle length, the number of days of heavy bleeding, how often you change protection and whether you pass clots gives your gynaecologist valuable clinical information. Noting associated symptoms such as pelvic pain, bloating or fatigue helps build a complete picture before your appointment.
Check your iron levels
If you have experienced heavy periods for several months, a blood test to check your full blood count and iron levels is worthwhile. Treating iron deficiency alongside managing menstrual bleeding significantly improves energy and overall wellbeing.
Seek specialist assessment
A private gynaecology assessment typically includes a full history, pelvic examination and a transvaginal ultrasound scan to identify structural causes such as fibroids or polyps. Blood tests to assess hormone levels, thyroid function and iron stores are also arranged. This gives a clear diagnosis and forms the basis of a personalised treatment plan, usually within a single appointment.
Get a private assessment at Ovara Health →
How do I stop heavy periods?
There is no single answer because treatment depends on the underlying cause, your age, whether you wish to preserve fertility and the severity of your symptoms. Options range from simple medication to minimally invasive procedures.
Non-hormonal medication
Tranexamic acid reduces menstrual blood loss by helping blood to clot more effectively at the site of bleeding. It is taken only during the days of heavy flow and does not affect fertility. Mefenamic acid, a non-steroidal anti-inflammatory, can also reduce blood loss and relieve associated period pain. Both are effective first-line options for women who prefer to avoid hormonal treatments.
Hormonal treatments
The combined oral contraceptive pill regulates the menstrual cycle and typically reduces blood loss significantly. Progestogen-only options including the mini-pill and injectable contraceptives can lighten periods in many women, though irregular spotting is common in the first few months.
The Mirena coil
The Mirena intrauterine system is one of the most effective treatments for heavy periods. This small hormonal device is fitted inside the uterus and releases a low dose of progestogen locally, thinning the uterine lining and dramatically reducing or stopping menstrual bleeding in the majority of women. It also provides highly effective contraception and lasts up to five years.
GnRH analogues
Gonadotrophin-releasing hormone analogues temporarily suppress ovarian function and stop periods. They are highly effective but generally used short-term due to side effects including menopausal symptoms and effects on bone density. They are most commonly used before surgery to shrink fibroids or reduce bleeding before a procedure.
Endometrial ablation
Endometrial ablation is a minimally invasive procedure that destroys the lining of the uterus, significantly reducing or stopping menstrual bleeding. It is suitable for women who have completed their family and whose heavy bleeding is not primarily caused by large fibroids. Most women return to normal activities within a few days of the procedure.
Treatment options at a glance
How do I stop heavy menstrual bleeding with clots?
Passing blood clots during a period is a sign that bleeding is heavier than normal. Clots form when menstrual blood pools faster than the body’s natural anticoagulants can break it down. While occasional small clots can be normal, larger or more frequent clots warrant investigation.
What clots indicate
Clots larger than a 50p coin, or clots passed repeatedly across multiple cycles, may suggest fibroids, adenomyosis or an endometrial abnormality. Clots are also more common during perimenopause as hormonal fluctuations cause the uterine lining to build up unevenly before shedding.
Treatment for clot-related bleeding
Tranexamic acid is particularly effective for reducing clot formation by promoting clotting at the site of bleeding. If fibroids are identified as the cause, treatment targeting the fibroids directly — such as the Mirena coil, uterine artery embolisation or myomectomy — addresses the underlying issue rather than just managing symptoms.
Why is my period so heavy this month?
A one-off heavy cycle is not unusual and is often caused by temporary factors. Understanding what has changed and monitoring your pattern over the following months is the sensible approach.
Common temporary causes
Stress, significant weight change, recent illness, travel across time zones and changes in medication can all alter menstrual flow in a given month. Some women notice a heavier period following a short gap between cycles or after a period of intense physical activity. These changes are usually self-resolving within one or two cycles.
When to investigate
If heavy bleeding recurs across two or more consecutive cycles, or if it represents a clear change from your normal pattern, investigation is recommended. A sudden increase in flow accompanied by pelvic pain, bleeding between periods, pain during sex or a feeling of pelvic pressure should be assessed promptly rather than monitored at home.
Heavy periods after 40 with clots — what you need to know
A change in your periods in your 40s is common, but it should not automatically be attributed to age or perimenopause without a proper assessment. Significant changes in bleeding pattern at this stage of life need to be investigated to exclude structural causes.
Perimenopause and changing periods
As ovarian function begins to decline in the years before menopause, oestrogen and progesterone levels fluctuate unpredictably. Cycles may become irregular, longer, shorter, lighter or much heavier. Clots become more common as the uterine lining may build up unevenly during cycles where ovulation does not occur.
Ruling out other causes
Even when perimenopause is the likely explanation, fibroids, polyps and endometrial thickening are more common in women over 40 and must be excluded. An ultrasound scan provides a clear picture of the uterus and ovaries and is the standard first investigation in this age group. Any woman over 45 with a new pattern of heavy or irregular bleeding should have her endometrial thickness assessed.
Treatment options in your 40s
The Mirena coil is particularly well suited to women in their 40s. It both treats heavy bleeding and provides effective contraception during a time when pregnancy, while less likely, remains possible. It can also be used as the progestogen component of HRT when the menopause transition is complete, making it a practical long-term solution for this age group.
When to call 999 or go to A&E: Seek immediate emergency care if you are soaking through a full pad or tampon every 15 to 30 minutes for two or more hours, if you feel faint or dizzy, if you have severe pelvic pain, or if you have unusual discharge or signs of infection alongside heavy bleeding. These may indicate a gynaecological emergency requiring urgent assessment.
What is the best treatment for heavy periods?
There is no universal best treatment. The right approach depends on the cause of your heavy bleeding, your age, whether you wish to preserve fertility and how severely your symptoms are affecting your daily life.
Personalised assessment first
Effective treatment starts with an accurate diagnosis. Without knowing whether fibroids, adenomyosis, hormonal factors or another cause is responsible, any treatment is a best guess. A specialist assessment with ultrasound provides the clinical foundation for targeted and effective management.
Minimally invasive and fertility-preserving options
For women who wish to preserve fertility, options include the Mirena coil, hormonal or non-hormonal medication, and — where fibroids are the cause — myomectomy or uterine artery embolisation. These approaches address the cause or control symptoms without removing the uterus.
Definitive treatment when needed
For women who have completed their family and have severe symptoms that have not responded to other treatments, endometrial ablation or hysterectomy may be considered. These are definitive solutions with high satisfaction rates but are not appropriate as a first-line approach in most cases.
Frequently asked questions about heavy period treatment
What is the clinical definition of heavy menstrual bleeding?
Heavy menstrual bleeding is clinically defined as blood loss of more than 80ml per cycle or bleeding lasting longer than seven days. In practice, any bleeding that disrupts daily activities, requires changing protection every one to two hours or involves passing large clots is considered clinically significant and warrants assessment.
Can heavy periods be a sign of cancer?
In the majority of cases heavy periods are caused by benign conditions such as fibroids, hormonal imbalance or adenomyosis. However, endometrial cancer can present with abnormal uterine bleeding, particularly in postmenopausal women or those over 45 with a new pattern of heavy or irregular bleeding. Any significant change should be assessed to exclude serious causes.
How quickly can heavy periods be treated?
Once a cause is identified, treatment can often begin promptly. Non-hormonal medication such as tranexamic acid can be started in the same cycle. The Mirena coil can typically be fitted within a few weeks of assessment. Minimally invasive procedures such as endometrial ablation are usually arranged within weeks of a decision to proceed.
Will the Mirena coil stop my periods completely?
Around 20 to 25 percent of women who have the Mirena fitted will have no periods at all after 12 months. The majority experience a significant reduction in blood loss. Some women have light irregular spotting in the first three to six months after fitting, which usually settles with time.
Can I treat heavy periods without hormones?
Yes. Tranexamic acid and mefenamic acid are both non-hormonal options that can significantly reduce menstrual blood loss. They are taken only during the days of heavy bleeding and do not affect fertility. Endometrial ablation is also a non-hormonal procedure that effectively reduces or eliminates periods in most women.
What investigations are done for heavy periods?
The standard initial investigation is a transvaginal ultrasound scan to assess the uterus, endometrial lining and ovaries. Blood tests check for anaemia, iron deficiency, thyroid function and hormone levels. In some cases a hysteroscopy is recommended to look directly inside the uterine cavity if a polyp or other abnormality is suspected.
What happens at a private gynaecology appointment for heavy periods?
At Ovara Health, an initial appointment with Mr Amer Raza includes a full clinical history, examination and where appropriate an ultrasound scan during the same visit. This means most women leave with a working diagnosis and a clear management plan after a single appointment, without waiting separately for a scan.
Can anaemia caused by heavy periods be treated?
Yes. Iron deficiency anaemia from heavy periods is treatable with oral iron supplements in most cases. Where anaemia is severe or oral iron is not tolerated, intravenous iron infusion provides a faster and more effective alternative. At Ovara Health both are available, and treating anaemia is considered alongside managing the underlying cause of the heavy bleeding.
What is the difference between heavy periods and abnormal uterine bleeding?
Heavy periods refer to excessive blood loss within a regular menstrual cycle. Abnormal uterine bleeding is a broader term covering any bleeding that is irregular in timing, frequency or amount, including bleeding between periods, after sex or after the menopause. Both warrant specialist assessment.
Do I need a GP referral to see Mr Amer Raza at Ovara Health?
No. You can book directly with Mr Amer Raza at Ovara Health without a GP referral. This means you can access specialist assessment, investigation and treatment promptly, without waiting for a referral letter.
Will my health insurance cover heavy period treatment?
Many private health insurance policies cover gynaecology consultations, investigations and treatment. Ovara Health works with most major insurers including Bupa, AXA Health, Aviva, Vitality, WPA and CIGNA. Contact your insurer to confirm your policy covers outpatient gynaecology before booking.
How do I know if my heavy periods are caused by fibroids?
Fibroids are typically identified on a transvaginal ultrasound scan. If you have heavy periods accompanied by a feeling of abdominal fullness, frequent urination, pelvic pressure or pain during sex, fibroids are a likely cause. An ultrasound scan at your first appointment will confirm or exclude this diagnosis.
Sources
- National Institute for Health and Care Excellence. Heavy menstrual bleeding: assessment and management. NICE guideline NG88. Updated 2021.
- NHS. Heavy periods. Accessed June 2026.
- Royal College of Obstetricians and Gynaecologists. Heavy periods patient information leaflet. Accessed June 2026.
Medical disclaimer: The information on this page is for general informational purposes only and does not constitute medical advice. It should not replace professional medical assessment, diagnosis or treatment. Always consult a qualified healthcare professional about any medical concerns. If you are experiencing a medical emergency, call 999 or attend your nearest A&E immediately.
Book Online
Call Us: 0207 751 4488
Request a Callback